Friday, September 23, 2005
Surgery Details
 We had our pre-op appointment today at the Children's Hospital. It went pretty well. We went over medical history and met with the surgeon. They got weight, height, and vitals. They also did chest x-rays, they took blood and urine, and did an EKG.
We had our pre-op appointment today at the Children's Hospital. It went pretty well. We went over medical history and met with the surgeon. They got weight, height, and vitals. They also did chest x-rays, they took blood and urine, and did an EKG.Sophia was pretty fussy and tired by the end. We were there 4.5-5 hours.
Like I said, we met with the surgeon and some of his staff. I thought I would post some diagrams of Sophia's heart and try to relay the details of the surgery. Here is a link regarding normal heart anatomy to use as a reference.
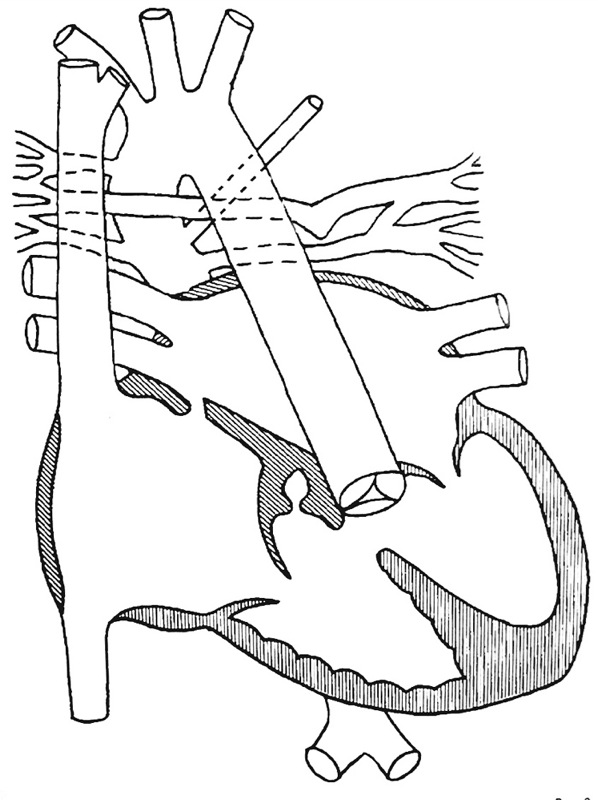
The line diagram to the left is what Sophia's heart was like at her first catheterization. In other words, there is no repair in this image.
Things to note:
If you look at the lower left chamber of the heart (the right ventricle or RV), the pulmonary valve is incomplete and does not connect to the pulmonary arteries (PA). This is called pulmonary trunk atresia. Also there is a substantial hole just below and to the right of the missing valve. This is called a VSD or ventricular septal defect. You might also notice tangled amongst the aorta and existing PAs, there are several small vessels that are connected in various places between the aorta and the lungs. These are called MAPCAs or multiple aorto-pulmonary collateral arteries. And if you are really perceptive you will notice the aortic arch is reversed from its normal direction.
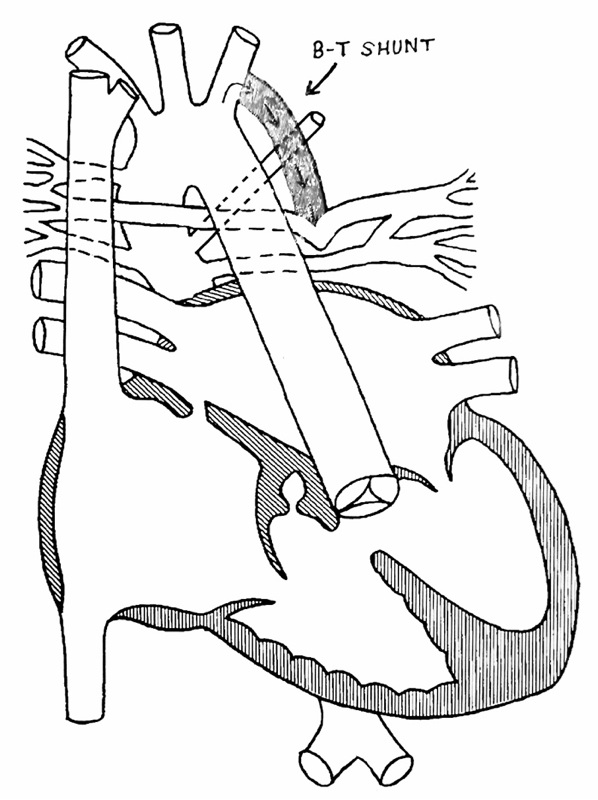
The next image shows the first repair called a Blalock-Taussig Shunt. This was done in November 2004, and I have written about it in a previous post. The repair is shown in gray. The purpose of this repair was to redirect the blood, returning to the body through the aorta, back to the lungs through the PAs (shaped like a seagull).

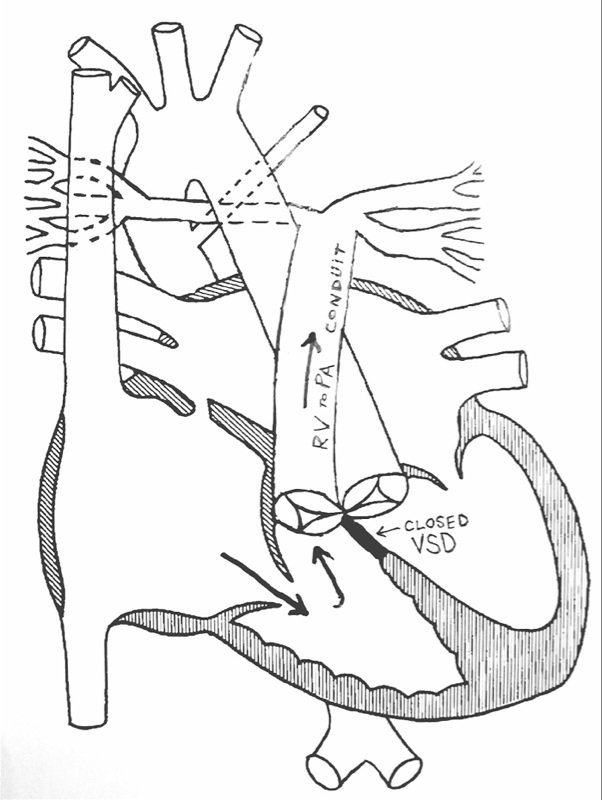
With the repair on Monday, the shunt will be removed and a conduit will be placed from the right ventricle to the pulmonary arteries.
This is called a RV to PA conduit. It is sourced from a cadaver donor. It will have a valve that allows the blood to flow in only one direction. This is not a permanent repair in the same way the shunt was not. Though it approximates the natural anatomy of the heart, Sophia will eventually outgrow it. There is also the possibility the valve will wear out. It should, however, last until age 7-10 given the valve lasts.
Also during the surgery, the MAPCAs will be unifocalized. This means they will be gathered together and connected to the PAs to allow them to bring blood to the lungs. In Sophia's situation these vessels are not servicing any part of the lungs that the PAs do not reach. This makes it less crucial they all be used. But, the surgeon is going to try to use them all.
Finally, the surgeon is going to either reduce or close the VSD. This will depend on the size and condition of the PAs and MAPCAs. Let me try to explain.
Because of the existing defects, the right ventricle has to pump pretty aggressively to move blood where it needs to go. With the repair, all that pressure will be directed to the PAs. If they are too small, the pressure could cause problems for the repair. In this case, the VSD offers a sort of relief valve. If it is necessary to have this relief the VSD will be reduced, if not the VSD will be closed. If the VSD were not closed, I am not sure if they would close it until they needed to repair the conduit later.
Below is an estimation of Sophia's heart after the repair.
 We are to arrive at the hospital at 6am on Monday. Surgery will be at 7:30. Anesthesia will put Sophia under using gas. She will then get 2 I.V. lines and an arterial line. They will put a breathing tube through her nose and into her windpipe. Then she will be hooked to a ventilator and the rest of the anesthesia will be administered. After this, the surgery will begin. It should last 4-6 hours.
We are to arrive at the hospital at 6am on Monday. Surgery will be at 7:30. Anesthesia will put Sophia under using gas. She will then get 2 I.V. lines and an arterial line. They will put a breathing tube through her nose and into her windpipe. Then she will be hooked to a ventilator and the rest of the anesthesia will be administered. After this, the surgery will begin. It should last 4-6 hours.Some of the concerns related to the surgery are outlined below. First, there is likely lots of scar tissue from her first surgery. This will have to be removed in order to give the surgeon access to the heart. This is of course a bleeding risk.
Another major risk is the heart/lung bypass. This is a machine that does the work of the heart and lungs while the heart is stopped for the surgery. This machine creates a sort of shock to these systems. And as a result there is much swelling and spilling of fluids into the tissues of the body.
Beyond that there are many other risk associated with the mechanics of the surgery and other general O.R. risks. We were told the risk of death is about 10%. This is obviously not as low as we would like. But the benefits far out weigh the risks.
This is a very general sketch of the procedure. And of course, not being a doctor myself, I am doing my best to be accurate. I will however make some errors in communicating this stuff. I will post more details as they are available. But, I wanted to give everyone an idea of what was going to happen. Check back after surgery, Monday night, I will try to post regarding the outcome.
-Michael
Comments:
<< Home
So many prayers, so many cares,how can anything go wrong when so much love abounds. People all over the world are praying for our precious dolly. Monday will show us how much this wonderful surgeon can accomplish.See you in the waiting room. I love you Mike, Patty and my precious dolly.
# posted by  : 9/24/2005 7:46 PM
: 9/24/2005 7:46 PM
: 9/24/2005 7:46 PM
found your blog while searching for VSD. Our son Sam was born with a "very large" VSD and tiny ASD. The VSD needed surgery and is detailed on our blog all-about-sam.
Our prayers are with you. We are 7 weeks post-surgery now.
Post a Comment
Our prayers are with you. We are 7 weeks post-surgery now.

<< Home
![]()




{kind=link}